For Affordable Care Act/Health Enrollments (2026)
Before completing your enrollment, please review the following attestation.
____________________________________________________________________________________________________________________________________________________________________________________________________________
I attest that no one applying for health coverage on this application is incarcerated.
I attest that no member on the enrollment application has group coverage offered to them.
I give permission to the marketplace to access my tax returns for up to 5 years to verify my income for subsidy purposes.
By agreeing to the terms and conditions, you understand that [Name] refers to the Agent's Name: Luis Ortiz, [Email] refers to: [email protected], National Producer Number [ __________] and [Phone] refers to: (917) 549-0496
___________________________________________________________________________________________________________________________________________________________________________________________________________
I agree to have my information used and retrieved from data sources for this application. I have consent for all people I’ll list on the application for their information to be retrieved and used from data sources. However, if I revoke permission, I understand that I will be required to complete a federal application every year to confirm my income and subsidy eligibility.
I understand that if any information listed on this application changes, it is my responsibility to update the information with the federal marketplace. I understand that I can make changes by accessing my marketplace account online or by calling 1-800-318-2596. I further understand that a change in my information could affect eligibility for members of my household.
___________________________________________________________________________________________________________________________________________________________________________________________________________
I agree to allow to submit my healthcare.gov financial assistance and health insurance application on my behalf.
___________________________________________________________________________________________________________________________________________________________________________________________________________
I understand that changes may occur to my premium based on my subsidy eligibility results. I authorize any Licensed Agent affiliated with ZZ - Luis Ortiz ACA 2.0 to submit the application for enrollment and notify me of these changes via the email I provided on the application.
I understand that I’m required to provide true answers and that I may be asked to provide additional information, including proof of my eligibility for a Special Enrollment Period. If I don’t qualify, I may face penalties, including the risk of losing my eligibility for coverage.
___________________________________________________________________________________________________________________________________________________________________________________________________________
I authorize and consent that ZZ - Luis Ortiz ACA 2.0 or one of its affiliated licensed agents will be my agent of record.
I authorize them to submit and sign this application on my behalf and use 3rd party verification tools to confirm my eligibility requirements (such as date of birth, Social Security number, address, legal name, etc.). I also authorize them to update my existing marketplace application and process my renewal applications unless I revoke this authorization. This consent will remain in effect until 11/1/35 unless I revoke it earlier.
You request that we make sure we are the Agent of Record on your account each month until consent is revoked. We will also make sure your application is up to date for Open Enrollment each plan year. If your current plan is discontinued, we will enroll you in the best plan you qualify for. If your eligibility changes, you are required to let us know. This permission may be rescinded at any time by emailing .
___________________________________________________________________________________________________________________________________________________________________________________________________________
I understand that because the premium tax credit will be paid on my behalf to reduce the cost of health coverage for myself and/or my dependents:
• I must file a federal income tax return in 2027 for the tax year of 2026.
• If I'm married at the end of 2026, I must file a joint income tax return with my spouse.
___________________________________________________________________________________________________________________________________________________________________________________________________________
I also expect that:
• I am not currently enrolled in Medicare or any State Medicaid Program.
• No one else will be able to claim me as a dependent on their 2026 federal income tax return.
• I’ll claim a personal exemption deduction on my 2026 federal income tax return for any individual listed on this application as a dependent who is enrolled in coverage through this marketplace and whose premium is paid in whole or in part by advance payments.
If any of the above changes, I understand it may impact my ability to get a premium tax credit.
___________________________________________________________________________________________________________________________________________________________________________________________________________
I also understand that:
• When I file my 2026 federal income tax return, the IRS will compare the income on my tax return with the income on my application.
• If the income on my tax return is lower than the income on my application, I may be eligible to get an additional premium tax credit.
• If the income on my tax return is higher than the income on my application, I may owe additional federal income tax.
I’m agreeing to this application under penalty of perjury, which means I’ve provided true answers to all the questions to the best of my knowledge. I understand that I may be subject to penalties under Federal law if I intentionally provide false information.
___________________________________________________________________________________________________________________________________________________________________________________________________________
If you got premium tax credits in 2024 or 2025, you agree that you filed a tax return with Form 8962 for at least one of those years.
___________________________________________________________________________________________________________________________________________________________________________________________________________
I agree that I have read this, and I give my permission to and ZZ - Luis Ortiz ACA 2.0 on 07/23/2026 to serve as my broker for myself and my household, for the purpose of enrollment in a qualified Health Plan offered by the Federally Facilitated Marketplace.
I consent to allow the above-mentioned agent to view and use my confidential information for the following purposes:
1. Search for an existing Marketplace Plan
2. Complete an application for eligibility and enrollment in a Marketplace Plan
3. Provide ongoing maintenance and enrollment assistance
4. Respond to inquiries from the Marketplace regarding my application
___________________________________________________________________________________________________________________________________________________________________________________________________________
If your income is $0 (or less than the Federal Poverty Limit), you attest that your estimated income for 2026 will be at least the Federal Poverty Limit for your state and household size.
If your income will be less than (or greater than) those limits, you agree to notify us or the marketplace of any changes or updates as soon as possible. Failure to notify us of any changes may result in your eligibility being affected.
___________________________________________________________________________________________________________________________________________________________________________________________________________
Job Seeking: I agree to notify if my estimated income for 2026 changes.
___________________________________________________________________________________________________________________________________________________________________________________________________________
By clicking the button/checking the box/attesting yes/signing, you are agreeing to this document. You attest to the accuracy of all statements on this page.
___________________________________________________________________________________________________________________________________________________________________________________________________________
You may revoke this consent by sending us an email at .
___________________________________________________________________________________________________________________________________________________________________________________________________________
I agree to have check and make sure I'm the Agent of Record at the end of each month. I do not consent to another agent taking over as my Agent of Record unless I revoke consent by emailing [email protected].
___________________________________________________________________________________________________________________________________________________________________________________________________________
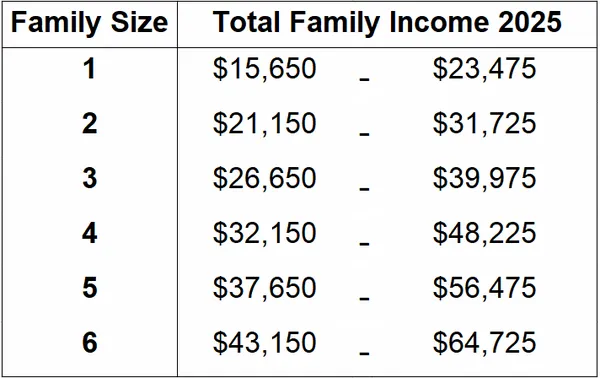
You agree that your income estimation would fall in the range below based on your tax household size.
___________________________________________________________________________________________________________________________________________________________________________________________________________
Total Amount of Direct Commission:
We typically receive $25–$30 (or less) per member we enroll per month they stay enrolled.